Hemorrhoid Treatment and Classification
Hemorrhoids are defined as an abnormal swelling or enlargement of the anal vascular cushions and are one of the most common causes of rectal bleeding. Although they often go away on their own, hemorrhoid treatments can also help. Here we will discuss how hemorrhoids are classified and the treatment options available today.
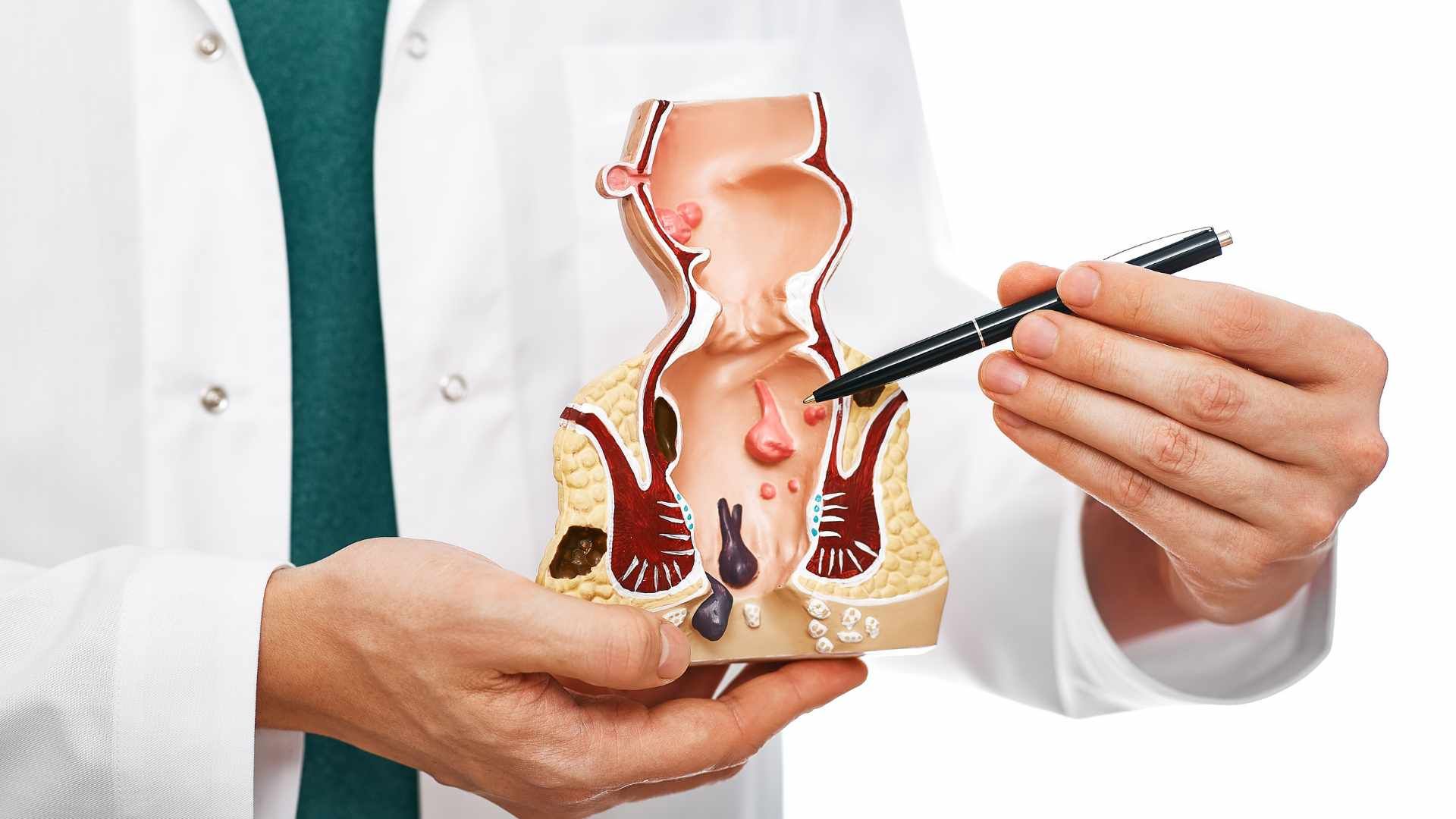
Hemorrhoids are classified relative to their relationship to the dentate line:
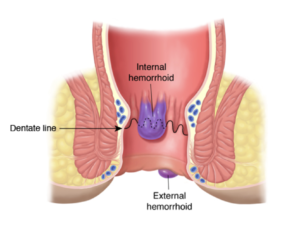
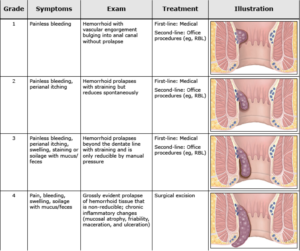
- Internal hemorrhoids are proximal to or above the dentate line. Tissues above the dentate line receive visceral innervation, which is less sensitive to pain and irritation. Thus, internal hemorrhoids are amenable to a variety of office-based procedures that can be carried out with minimal or no anesthesia. Internal hemorrhoids are further sub classified into four grades based on the degree of prolapse from the anal canal.
- External hemorrhoids are distal to or below the dentate line, where tissues are innervated somatically, and therefore are more sensitive to pain and irritation. As a result, symptomatic external hemorrhoids that are refractory to conservative management are generally treated surgically under anesthesia, with the exception of small, acutely thrombosed external hemorrhoids, which can sometimes be treated in the office.
- Mixed internal and external hemorrhoids straddle the dentate line and are generally treated in the same way as are external hemorrhoids.
For all patients with gastroenterology conditions such as symptomatic hemorrhoids, we recommend initial conservative treatment with dietary management consisting of adequate fluid and fiber intake.
- Most patients with low-grade (I or II) internal hemorrhoids respond favorably to conservative treatment and do not require any further treatment. Reasons to refer patients to a specialist, like a gastroenterologist , include refractory or complicated hemorrhoids for possible intervention and rectal bleeding for possible colonoscopy.
- For patients with grade I, II, or III internal hemorrhoids refractory to conservative treatment, we recommend an office-based procedure, rather than surgical hemorrhoidectomy, as the initial intervention. Compared with surgical treatment of hemorrhoids, most office-based procedures cause less pain and less complications.
- Commonly performed office-based procedures include rubber band ligation, sclerotherapy, and infrared coagulation of internal hemorrhoids.
- For healthy patients with grade I, II, or III internal hemorrhoids, we recommend rubber band ligation rather another office-based procedure. Compared with sclerotherapy or infrared coagulation, rubber band ligation is more effective and requires fewer treatment sessions.
- Rubber band ligation is contraindicated in patients who are on anticoagulant or antiplatelet drugs, are immunocompromised, or have portal hypertension. In these patients, we suggest sclerotherapy rather than infrared coagulation. Sclerotherapy is better studied in these patients.
- Patients with grade IV internal hemorrhoids, those with combined internal and external hemorrhoids and significant prolapse, and those with another indication for anorectal surgery should be offered surgical hemorrhoidectomy if they fail conservative treatment.
- Acutely thrombosed external hemorrhoids can be treated by office-based excision if the patient presents within the first three days of symptoms. The symptoms usually begin to subside after three days and typically dissipate in 7 to 10 days. Extensive or bleeding thrombosed external hemorrhoids may require surgical excision in the operating room.
Source: Uptodate ®
Learn More About Hemorrhoid Treatments
About Hemorrhoid Treatments Symptoms And Diagnosis
What Causes Hemorrhoids
The Crh Oregan System Hemorrhoid Treatment
The post Hemorrhoid Treatment and Classification appeared first on Gastro SB.