Patient Education: When to See a Gastroenterologist for an Anal Fissure (Beyond the Basics)
ANAL FISSURE OVERVIEW
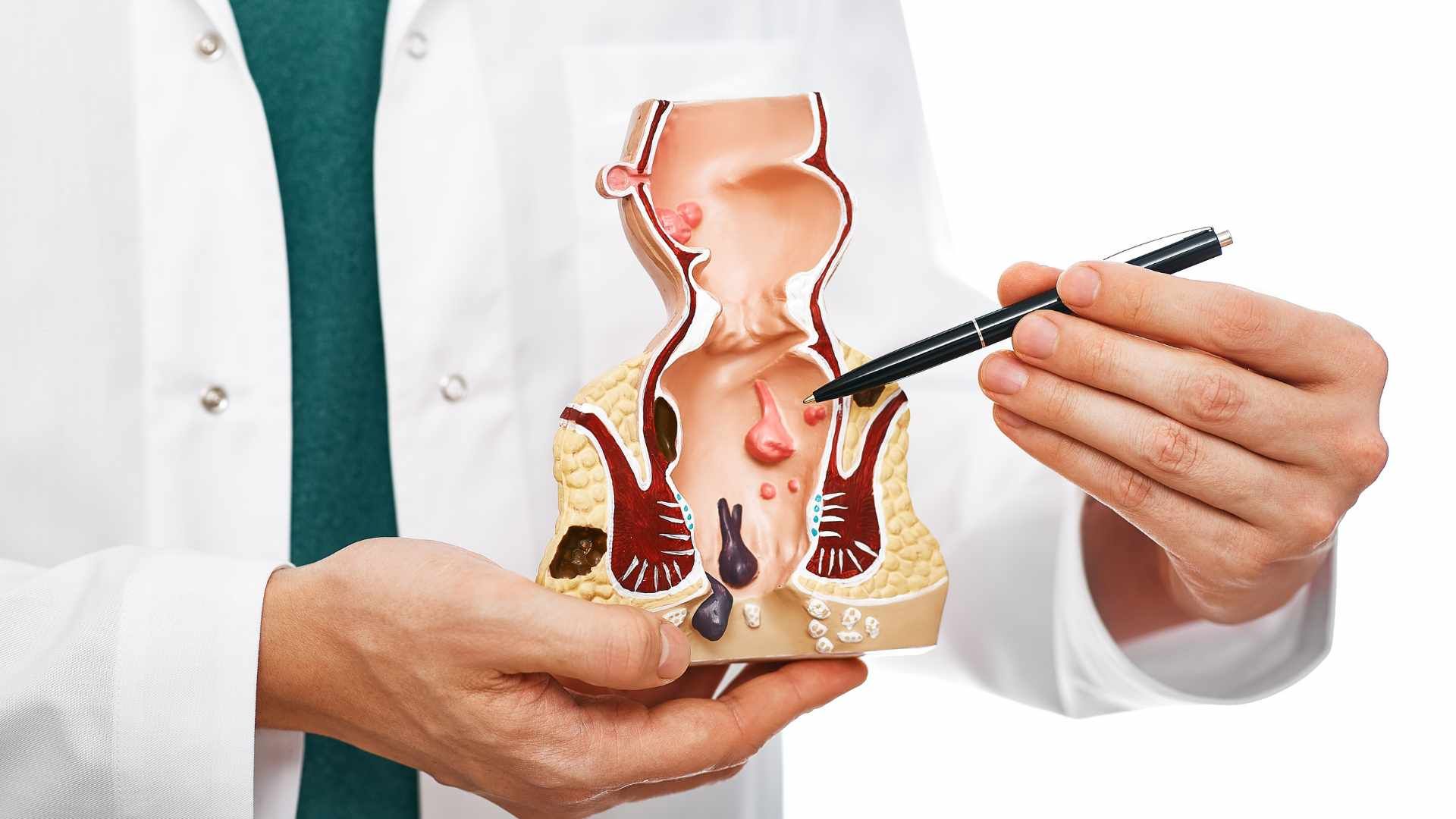
An anal fissure is a tear in the lining of the anus, the opening where feces are excreted. The tear typically extends into a circular ring of muscle called the internal anal sphincter. The fissure is described as acute if it has been present for less than six weeks or chronic if present for more than six weeks. Anal Fissures can be best diagnosed by a gastroenterologist. Anal fissure anatomy
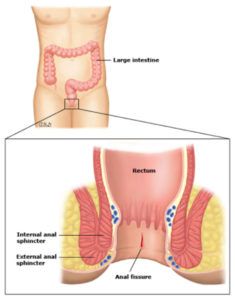
Once a fissure develops, the internal anal sphincter typically goes into spasm, causing further separation of the tear, constricting blood flow to the area, impairing healing, and causing pain.
There are no reliable estimates of the frequency of anal fissures in the general population; some studies suggest that as many as one in five persons develop a fissure during their lifetime. This may be an underestimate since some people may be too embarrassed to discuss it with their healthcare provider.
ANAL FISSURE SYMPTOMS Patients with an anal fissure may first note bleeding and a sensation of tearing, ripping, or burning following a bowel movement. Once a fissure develops, these symptoms can occur after every bowel movement; the rectal pain can be severe and can last several minutes to hours.
Bleeding is usually of a small volume, though it is often bright red. However, the bleeding may discolor the toilet bowl, giving it the appearance of heavy bleeding. Some patients also note itching or irritation of the skin around the anus.
ANAL FISSURE CAUSES AND RISK FACTORS Anal fissures are usually caused by trauma that stretches the anal canal, such as after passage of large or hard bowel movement or explosive diarrhea.
Less commonly, fissures are caused by foreign body insertion or anal intercourse. Anal fissures can also occur in patients who have other GI symptoms or medical conditions such as Crohn disease (an inflammatory disease of the intestines). As a result, part of the evaluation may include testing for these conditions.
ANAL FISSURE DIAGNOSIS Anal fissures can usually be diagnosed based on the symptoms described above and a physical examination. The physical examination involves gently separating the buttocks, allowing for visual inspection of the region around the anus. A fissure most commonly appears in the 12 or 6 o’clock position. Fissures located in other locations are more likely to be associated with an underlying disorder (eg, Crohn disease).
A rectal examination (insertion of a gloved finger into the anus) or anoscopy (insertion of a small instrument to view the anal canal) can often be avoided in the initial diagnosis of a fissure. These examinations can cause increased pain and are often unnecessary to establish a provisional diagnosis based on history and visual examination. Further evaluation may be required if there is concern that another medical condition may have contributed to the development of the fissure.
If the diagnosis is unclear, a sigmoidoscopy or colonoscopy is usually recommended, especially if there has been rectal bleeding. A colonoscopy is preferred in patients 50 years and older and can also be used to screen for colorectal cancer. In younger patients with no risk factors for colorectal cancer or intestinal diseases, a sigmoidoscopy may suffice.
ANAL FISSURE TREATMENT Medical and surgical treatments are aimed at reducing the tone of the internal sphincter muscle, leading to pain relief and healing of the anal fissure. People with a new anal fissure may resolve this ailment without medical treatment, though a higher rate of cure is associated with treatment by a physician. By contrast, those with a chronic anal fissure usually require medical intervention.
Initial treatment is medical and aimed at eliminating constipation, softening stools, and reducing anal sphincter spasm. There are several approaches to reducing anal sphincter spasm, which will be described below. These measures are successful in 60 to 90 percent of patients. However, some patients may not heal, or they may develop frequent recurrences. Such patients may require surgery, which is successful more than 95 percent of the time.
Fiber therapy — Avoiding hard bowel movements will prevent trauma to the anal canal, promoting healing of the fissure. Increasing fiber in the diet is one of the best ways to soften and bulk the stool. Fiber is found in fruits and vegetables. The recommended amount of dietary fiber is 20 to 35 g/day.
Fiber supplements are commercially available, including psyllium (Metamucil), methylcellulose (Citrucel), wheat dextrin (eg, Benefiber), and calcium plycarbophil (Fibercon). These products work by absorbing water and increasing stool bulk, which improves regularity of bowel habits while softening stools. Bulk-forming laxatives are very safe, but side effects may include gas and bloating, especially when they are first started. They may be used alone or in combination with dietary changes and are safe to use every day. Bulk-forming laxatives are not habit forming and can be used lifelong.
Laxatives — A variety of drugs and natural products are available for treating constipation.
People are often concerned about the regular use of laxatives, fearing that they will not be able to have a bowel movement when the laxative is stopped. However, with the exception of cathartic laxatives (such as senna-related products), there is little to no evidence that laxatives increase the risk of constipation in the future.
Topical nifedipine and topical nitroglycerin — Topical nifedipine works by reducing the internal anal sphincter pressure. Nifedipine is available in pill form for other indications (eg, to treat high blood pressure) but is best used for fissure treatment when compounded into a topical treatment and applied directly to the perianal skin. Topical treatment with 0.2 to 0.3% nifedipine two to four times a day has few side effects.
Nitroglycerin also results in a reduction in pressure of the internal anal sphincter, which decreases pain and further facilitates healing.
The dose of nitroglycerin is usually a small, pea-sized dot of 0.2 to 0.4% ointment applied around the anal opening two times daily. The lower strength of nitroglycerin must be compounded (custom-made) by a pharmacist. The higher strength of nitroglycerin ointment is now available commercially as Rectiv. It is very important to use the correct strength and amount of nitroglycerin ointment to avoid side effects such as severe headaches. It is also important to wash the hands after applying the ointment.
Nitroglycerin side effects can include headache and low blood pressure. Headaches are generally mild, last less than 30 minutes, and resolve after two weeks of nitroglycerin use. Dizziness is another possible side effect; patients should sit or lie down to apply the ointment and should sit or stand up slowly. Nitroglycerin should not be used within 24 hours of medications used for erectile dysfunction, such as Viagra (sidenafil), Cialis (tadalafil), and Levitra (vardenafil). There is no risk of explosion with nitroglycerin ointment.
Botulinum toxin — Botulinum toxin is a neurotoxin produced by a bacterium, Clostridium botulinum. It temporarily paralyzes muscles for up to three months, and it can be injected into the internal anal sphincter muscle in a clinician’s office without anesthesia or sedation. The dose is extremely low and has virtually no risk of causing botulism poisoning. Botulinum can cause temporary, mild anal incontinence (leakage of gas or stool) in some patients (7 percent in one study) [ 1 ]. Because it involves an injection (rather than topical application), it is usually reserved for patients who do not respond to topical therapy.
Surgery — Surgical procedures are generally reserved for people with symptoms that have persisted despite medical therapy for at least one to three months. The procedure of choice is called a lateral internal sphincterotomy, which relaxes the internal anal sphincter by cutting this muscle. This is generally performed as an outpatient procedure while providing the patient a general anesthetic. Pain from the sphincterotomy is usually mild and is often less than the pain of the fissure itself. Patients often return to normal activity within one week.
The main concern with surgery is the development of fecal incontinence. Fecal incontinence can include the inability to control gas and/or stool. Mild incontinence in the form of anal seepage can occur in up to 45 percent of patients in the immediate postoperative period, and this may be mistaken by patients for permanent incontinence. However, this immediate postsurgical incontinence is rarely permanent and is usually mild. The risk for permanent incontinence should be discussed with your surgeon.
Comparison among surgery and nitroglycerin, botulinum toxin, and nifedipine or diltiazem reveals that surgery has a higher success rate. In one study, close to 100 percent of patients with fissure who underwent surgery were completely healed by two months after surgery. This compared to only 64 percent of patients who healed two months after botulinum toxin injections. However, the number of patients with complications (anal incontinence, infection) was higher in the surgical group, and the time it took patients to recover from surgery was longer than those who had injections. Similar results have been described in studies comparing botulinum toxin, nifedipine, and diltiazem to surgery.
Source: Update ®
Read More About How a Gastroenterologist Can Help
Gastroenterologist near me
How to Prep for a Colonoscopy
What is a Gastroenterologist
Fight the fatty liver with a gastroenterologist
How do you know when to see a gastroenterologist?
What is Hiatal Hernia?
Colon Cancer Q&A with a Gastroenterologist
What is a GERD and When Should You See a Gastroenterologist?
When to See a Gastroenterologist for an Anal Fissure
The post Patient Education: When to See a Gastroenterologist for an Anal Fissure (Beyond the Basics) appeared first on Gastro SB.